Diet & Nutrition on GLP-1
Summary: GLP-1 medications shrink appetite, so each meal has to do more nutritional work. The practical playbook is protein at every meal, steady fluids and fiber, smaller portions of high-fat or very sweet foods that tend to trigger nausea, and a careful hand with alcohol.
This content is for informational purposes only and is not medical advice. Always consult a qualified healthcare provider before starting, changing, or stopping any medication.
Why what you eat matters more on a GLP-1
GLP-1 receptor agonists like semaglutide and tirzepatide reduce appetite and slow gastric emptying, so most people end up eating noticeably less without trying. [1] In the STEP-1 trial of semaglutide 2.4 mg, average daily energy intake fell by roughly 35 percent within the first months of treatment, and similar or larger drops have been documented for tirzepatide. [2] When intake falls that fast, the composition of what you do eat starts to matter more, not less. A smaller plate has to deliver enough protein to protect muscle, enough fiber and fluid to keep your gut moving, and enough vitamins and minerals to avoid running a deficit over months of treatment. [2][9]
Weight loss from any source, GLP-1 included, is a mix of fat and lean tissue. Trial data and reviews suggest roughly 25 to 40 percent of total weight lost on GLP-1 therapy can come from lean mass if intake is poor and resistance training is absent. [3][10] A recent case series of patients who actually preserved or increased lean mass on semaglutide and tirzepatide reported daily protein intakes in the range of 0.7 to 1.7 g per kilogram of body weight, or 1.6 to 2.3 g per kilogram of fat-free mass, paired with three to five resistance-training sessions per week of about 15 to 45 minutes each. [11] The dietary side of that equation is the part you can control at every meal.
The other reality is that GLP-1 medications are appetite tools, not eating-skill tools. They make it easier to eat less, but they do not pick the foods, set the protein floor, or remember the water bottle. Most of the long-term outcome difference between people who do well and people who do poorly on these drugs comes down to a small number of repeatable habits: protein at every meal, fluid throughout the day, fiber on a slow ramp, movement most days, and a soft hand with foods and drinks that already make you feel rough. The rest of this guide walks through each of those, with specific numbers where the evidence supports them.
Protein first: targets and why it matters
Protein is the single most useful lever for protecting lean mass during GLP-1 weight loss. A reasonable working target for most adults is 1.2 to 1.6 grams of protein per kilogram of body weight per day, with the higher end favored for older adults, those losing weight rapidly, and anyone doing structured resistance training. [3][4][11] For a 75 kg adult that is roughly 90 to 120 g per day. People with significant obesity should generally calculate against ideal or goal body weight rather than current body weight to avoid an unrealistic protein number; a common dietitian shortcut is 0.6 to 0.8 g of protein per pound of goal weight. [12]
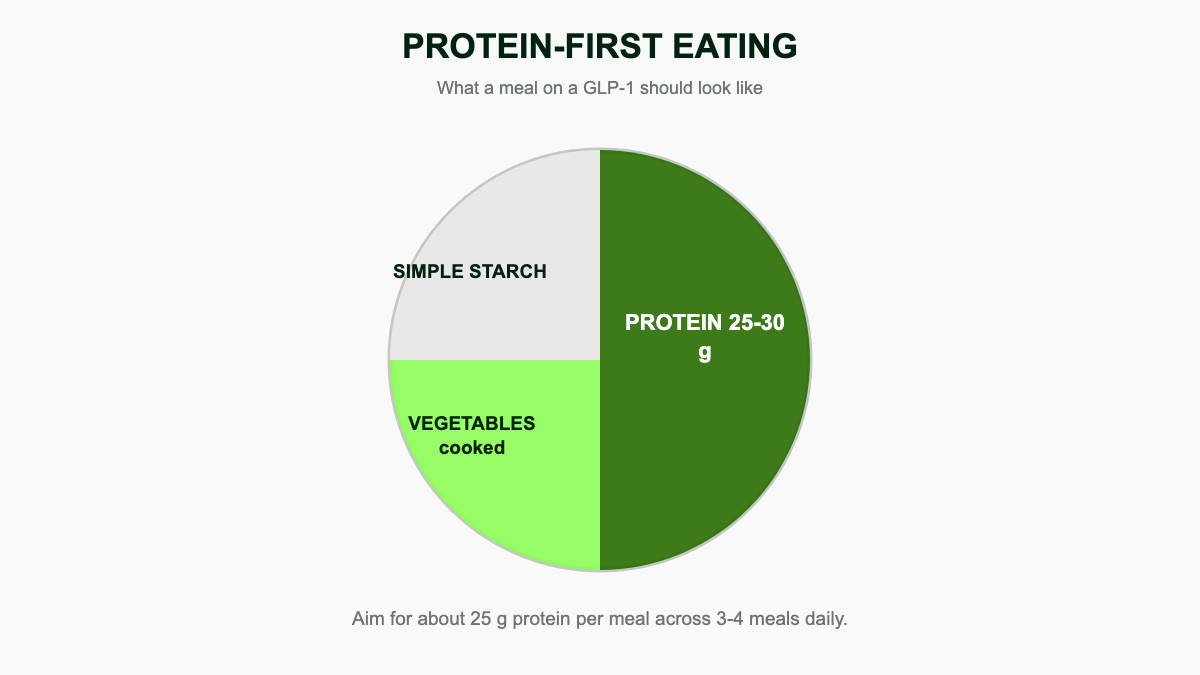
Distribution matters as much as the total. Muscle protein synthesis is driven by hitting a leucine threshold of roughly 2.5 to 3 g of leucine per meal, which corresponds to about 25 to 35 g of high-quality protein per sitting in adults, and 30 to 40 g per sitting in older adults whose anabolic response to protein is blunted. [4][12] In practice, that means front-loading protein at breakfast, where most people on a Western diet under-eat it, and aiming for a protein anchor at every meal rather than back-loading the day at dinner.
A simple per-meal target sheet looks like this:
- Breakfast: 25 to 35 g (eggs and Greek yogurt, cottage cheese on toast, protein oatmeal, a shake)
- Lunch: 25 to 35 g (chicken or tuna salad, lentil and feta bowl, turkey wrap, tofu stir-fry)
- Dinner: 25 to 35 g (baked fish, lean steak, chicken thigh, tempeh)
- Optional snack: 10 to 20 g (string cheese and edamame, jerky, a small protein shake, skyr)
Practical protein anchors that tend to be well tolerated on a slow stomach:
- Eggs and egg whites (about 6 g per large egg, 25 to 30 g in a three-egg omelet with cheese)
- Greek yogurt, skyr, and cottage cheese (15 to 25 g per cup)
- Chicken or turkey breast, baked or grilled (about 25 g per 3 oz)
- White fish, salmon, canned tuna in water, shrimp, and rotisserie chicken
- Tofu, tempeh, edamame, lentils, and chickpeas
- Whey, casein, or pea protein powders mixed into milk, yogurt, or oats
- Low-fat milk, unflavored kefir, and ricotta
- Lean deli turkey, lean roast beef, and high-protein jerky for portable options
If appetite is genuinely small, anchor each meal with the protein first, then add carbohydrates and produce around it. Many patients find a protein shake or skyr cup easier to finish than a full plate on dose-escalation weeks. A blended smoothie with milk or yogurt, frozen berries, a scoop of protein powder, and a tablespoon of nut butter or chia is often the easiest way to land 30 to 40 g of protein when nausea is at its worst. [5]
Plant-eaters can hit the same targets but usually need to combine sources at most meals because plant proteins tend to be lower in leucine per gram than animal proteins. [13] Tofu plus edamame, lentils plus seitan, or soy yogurt plus pea-protein powder are common pairings that get a meal up to the 25 to 30 g range with a more complete amino acid profile. Soy and pea isolate are the closest plant matches to whey for muscle synthesis. [12][13]
Foods that tend to worsen nausea
Nausea is the most common side effect of GLP-1 therapy, especially during dose increases, and it usually improves within a few weeks at a stable dose. [1][5] Because the stomach is emptying more slowly, foods that already sit heavily tend to sit even longer, and very rich or very sweet meals can trigger an outsize wave of queasiness, fullness, and reflux. The usual offenders, drawn from registered-dietitian guidance and patient survey data:
- Fried and very greasy foods: fried chicken, French fries, mozzarella sticks, deep-fried fish, heavy cream sauces, full-fat pizza
- Fatty cuts of meat in large portions (ribeye, ribs, fatty pork, full-fat ground beef, fatty bacon)
- Very sweet desserts, sugary drinks, juice, and rich pastries that can produce a sugar dump and nausea
- Spicy foods, for a meaningful subset of patients with heartburn or reflux
- Carbonated beverages, including diet sodas and seltzer, which trap gas in a slow stomach and worsen bloating and reflux [14]
- Alcohol, which compounds nausea, dehydration, and reflux (more on this below)
- Large raw cruciferous salads (raw broccoli, cauliflower, cabbage) that ferment slowly and can produce gas [14]
- Very large portions of any food, even healthy ones, which sit longer in a slow stomach
- Strong cooking smells; many patients tolerate cold or room-temperature foods better than hot, aromatic ones
- Eating quickly or to fullness rather than stopping early; aim for comfortable rather than satisfied
Lactose can become a hidden trigger on GLP-1s. Plenty of adults have low-grade lactose intolerance that they only notice once meals are smaller and digestion is slower; a glass of milk that used to be fine can suddenly cause cramping or loose stools. If dairy started bothering you only after starting a GLP-1, try a one-week swap to lactose-free milk, hard cheeses, and Greek yogurt (which is naturally lower in lactose) before assuming the medication itself is the problem. [9]
You do not have to ban any of these foods, and rigid food rules tend to backfire. The pattern that works for most people is smaller portions, slower pace, and stopping at comfortable rather than full. [5][6] If a specific food repeatedly triggers nausea, it is reasonable to drop it for a month and try reintroducing it at a higher tolerance later in treatment.
Foods that usually feel okay
When nausea is active, simple, lower-fat, lightly seasoned foods are the most reliable choices. The pantry list below is what most dietitians keep in their handouts for patients in the first months of treatment, and it doubles as a useful default shopping list for the rest of the year. [6][9][14]
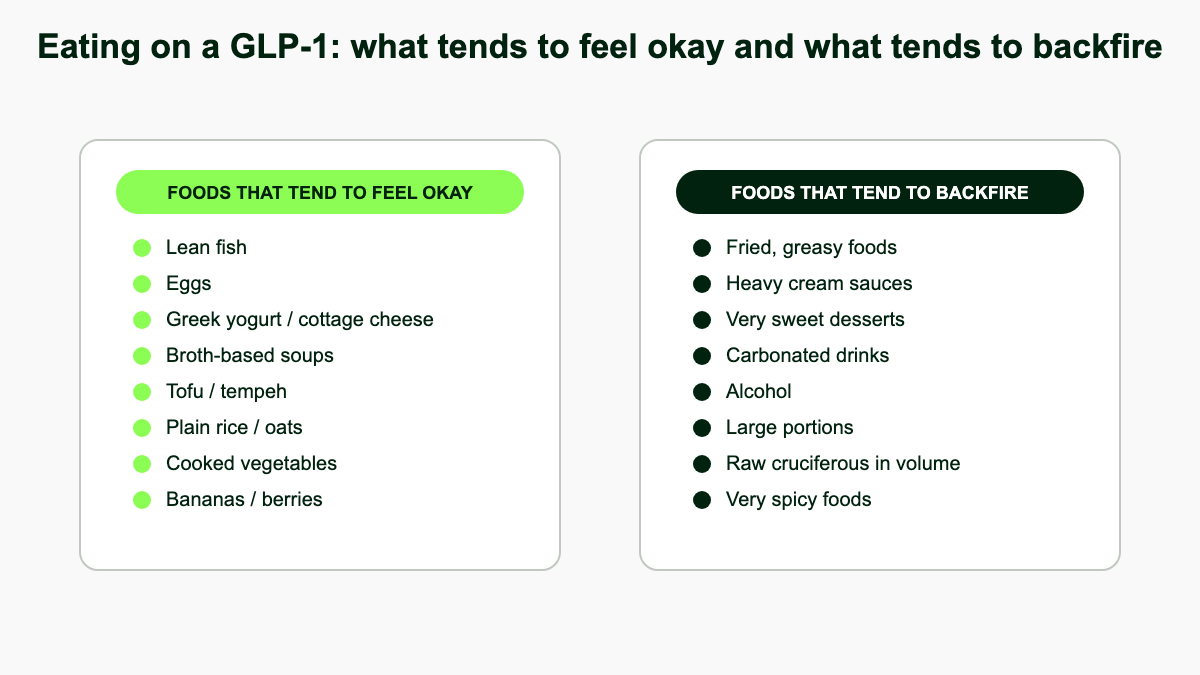
- Lean protein: grilled or baked chicken breast, baked white fish and salmon, eggs, Greek yogurt, cottage cheese, low-fat ricotta, tofu, tempeh, lentils
- Simple starches: rice, oats, potatoes, sweet potatoes, plain pasta, sourdough toast, crackers, polenta
- Broth-based soups (chicken and rice, miso, lentil, vegetable, chicken noodle), which are easy to sip and high in fluid
- Low-fat dairy, lactose-free milk, and unsweetened plant milks (soy and pea give the best protein per cup)
- Cooked vegetables: roasted carrots, zucchini, squash, green beans, spinach wilted in oil, sauteed peppers
- Soft fruits: bananas, melons, applesauce, peeled apples, ripe pears, papaya, mango
- Ginger tea, candied ginger, peppermint tea, plain water with lemon
- Cold or room-temperature foods (yogurt parfaits, hummus and pita, deli sandwiches, overnight oats), which often smell less strongly than hot meals
- Smoothies and protein shakes when chewing feels like too much work
A useful mental model is to think in terms of building plates that are protein-centered, gently cooked, and lightly seasoned. A grilled chicken breast with rice and roasted carrots will almost always sit better than the same calories from a creamy pasta dish. Eating something small every two to four hours tends to work better than waiting until you are hungry, because real hunger cues can be muted on GLP-1s and the empty-stomach-then-big-meal pattern is the single most common nausea trigger patients describe. [5][6]
Hydration, electrolytes, and avoiding the dehydration spiral
Hydration is the most under-managed single variable in GLP-1 nutrition. With less food coming in, you also pull in less water from food (food normally provides roughly 20 percent of daily fluid intake), and the appetite suppression that quiets hunger also quiets thirst signaling for many patients. The result is that people quietly drift into mild dehydration that shows up as headaches, fatigue, dizziness on standing, dark urine, sugar cravings, and worsening constipation. [6][9]
A reasonable baseline target is 2 to 3 liters of fluid per day from water, unsweetened tea, broth, milk, and water-rich foods, with more in heat, at altitude, or with exercise. [6] Useful warning signs that you are running low: urine darker than pale straw, urinating less than four times during waking hours, dizziness when you stand up quickly, persistent headaches, and dry mouth or lips. A simple practical anchor is to keep a 1-liter bottle visible at your desk and aim to refill it twice between waking and dinner.
Plain water alone is not always enough. If you are losing weight quickly, sweating in heat, exercising, or experiencing diarrhea, you are also losing sodium, potassium, and magnesium that water cannot replace. Drinking very large volumes of plain water on a low-sodium intake can in rare cases produce hyponatremia (low blood sodium), which presents as nausea, headache, confusion, and muscle cramps. [9] Reasonable electrolyte strategies for most patients include:
- Salting food to taste rather than aggressively under-salting (most people on calorie deficits do not need a low-sodium diet unless prescribed one for blood pressure or kidney reasons)
- Broth-based soups, miso, or bouillon once a day, especially if you are working out or in heat
- An unsweetened or lightly sweetened electrolyte mix (look for products with about 500 mg of sodium and 200 to 300 mg of potassium per serving) on heavy training days or when nausea has cut your food intake
- Coconut water, lower-sugar sports drinks, or homemade rehydration mixes (a quart of water, a quarter teaspoon of salt, and a tablespoon of honey or sugar)
- Foods naturally high in potassium (bananas, potatoes, oranges, beans, yogurt) and magnesium (leafy greens, nuts, seeds, whole grains)
If you take blood pressure medication or a diuretic, talk to your prescriber before adding daily electrolyte drinks, because the GLP-1 plus a smaller appetite plus aggressive sodium can occasionally push blood pressure or sodium in unwanted directions.
Constipation, fiber, and keeping the gut moving
Constipation is reported in roughly 10 to 25 percent of GLP-1 users in clinical trials and usually peaks during dose-escalation weeks before easing at a stable dose. [1] The mechanism is straightforward: gastric emptying is slower, total food volume is smaller, fluid intake often drops, and physical activity sometimes drops too. The good news is that the same handful of interventions resolves it for most patients. [6][14]
Fiber helps, but ramp it up slowly (5 g every few days) so it does not backfire as bloating, gas, and worse constipation. Aim for 25 to 35 g of total fiber per day, paired with the fluid targets above. [6][14] A useful split is roughly two-thirds soluble fiber and one-third insoluble fiber:
- Soluble fiber (forms a gel, softens stool): oats, chia seeds, ground flaxseed, psyllium husk, beans, lentils, ripe bananas, apples, oranges, sweet potatoes
- Insoluble fiber (adds bulk, speeds transit): wheat bran, whole-grain bread, brown rice, leafy greens, vegetable skins, nuts and seeds
- Specific high-yield foods: 2 to 4 prunes a day, 2 kiwifruit a day (a small randomized trial showed kiwi rivals psyllium for chronic constipation), 1 to 2 tablespoons of ground flax or chia in oats or yogurt
If food alone does not get you there, the supplement options most dietitians and gastroenterologists reach for first are well tolerated and not habit-forming:
- Psyllium husk: start at half a teaspoon mixed in 8 to 12 oz of water once a day, build to 1 to 2 teaspoons up to twice a day. Drink the full glass of water with each dose. [14]
- Magnesium citrate or magnesium oxide: 200 to 400 mg at night is a common starting dose for constipation; magnesium oxide tends to be the most laxative form. [14] Avoid if you have kidney disease without provider input.
- Polyethylene glycol (MiraLAX): 17 g once daily in water, well-studied and not habit-forming, often the first step for stubborn cases. [14]
- Stool softeners (docusate): helpful when stool is dry rather than slow.
- Senna: useful for occasional rescue but not as a daily long-term plan.
Daily walking moves the gut as much as any food does, and a 10 to 20 minute walk after meals is one of the highest-yield, lowest-effort interventions you can add. [6] Call your provider if you have gone more than a week without a bowel movement despite fluids, fiber, and an OTC laxative, or if you develop severe abdominal pain, persistent vomiting, or unrelenting bloating, which can occasionally signal a more serious issue such as obstruction or, rarely, gastroparesis. [14]
Alcohol on GLP-1s
Alcohol behaves differently on a GLP-1. Slowed gastric emptying changes how quickly alcohol is absorbed, and many patients report needing far less to feel intoxicated, more next-day nausea, and worse hangovers. [5][7] The change is large enough that the standard one-or-two-drink internal calibration most adults rely on can mislead them in the first months of treatment. A useful starting rule is to halve your usual amount, drink on a full stomach with water alongside, and reassess after the first sober morning.
The more interesting finding is that GLP-1 medications appear to reduce the desire to drink in the first place. A 2023 observational analysis by Quddos and colleagues showed meaningful reductions in alcohol consumption in semaglutide and tirzepatide users compared with matched controls, and a 2025 phase-2 randomized trial published in JAMA Psychiatry confirmed that low-dose semaglutide reduced both alcohol craving and the quantity consumed in adults with alcohol use disorder over a 9-week treatment period. [7][15] The proposed mechanism is reduced reward signaling in the brain's ventral striatum, the same circuitry implicated in food cravings, which is consistent with patient reports of "the drink just doesn't feel as good anymore."
Practical guidance:
- If you choose to drink, keep portions small (count drinks honestly, not by glass size) and never on an empty stomach
- Alternate every alcoholic drink with a glass of water
- Skip carbonated mixers if they trigger reflux; flat mixers tend to sit better
- Be especially careful with sugary cocktails, which can stack a sugar dump on top of alcohol's gastric effects
- Watch for next-day dehydration; alcohol plus a smaller appetite plus reduced thirst is a setup for a rough morning
- If you have a history of alcohol use disorder, mention it to your prescriber; the same craving-reduction effect that helps some patients can occasionally feel destabilizing for others
Meal patterns and timing
There is no single right pattern. What matters is that you eat enough, often enough, to hit your protein target without forcing food when you feel full. Two patterns work well in clinical practice:
- Three small meals plus one or two snacks, each anchored by 20 to 30 g of protein, for people who do better with structure or who work in offices with set lunch breaks
- Four to six mini-meals, each 200 to 400 kcal, for people whose stomach simply will not accept a full plate, especially during dose-escalation weeks or on the day of a higher-dose injection
Skipping meals tends to backfire on GLP-1s. You rarely make up the calories or protein later in the day, and rebound nausea is common when an empty stomach finally meets food. [5] If you genuinely cannot eat in the morning, prioritize fluid and a small protein-forward bite (a Greek yogurt cup, a half-shake, a hard-boiled egg) so the gut is not completely empty, then build into a real lunch.
Meal timing also matters more than people expect. Some patients find that nausea peaks in the late afternoon or evening, which is a useful argument for an early dinner and a front-loaded eating window. Others find injection-day nausea is worst in the first 24 to 48 hours, in which case it is reasonable to plan that window around easier foods (broth, soup, smoothies, yogurt) and save heavier social meals for later in the week. Many patients now schedule injections on a Friday night so the worst symptom window lines up with weekend rest, then return to a full eating pattern by Monday.
One more pattern worth flagging: front-loading protein at breakfast. Several short studies of higher-protein breakfasts in adults with overweight have shown better day-long satiety and lower evening snacking. [12] On a GLP-1, where appetite is naturally smaller in the evening anyway, getting 30 g of protein in by 10 a.m. (eggs, Greek yogurt with berries, cottage cheese on toast, or a high-protein smoothie) is one of the easiest ways to make the daily protein target without having to force a heavy dinner.
Sample meal plans
The plans below are templates rather than prescriptions, built to land roughly on protein targets at three common calorie levels. Adjust portions to your hunger, body size, and any conditions a registered dietitian is already managing for you. Calories are approximate.
1,200 to 1,400 kcal day, around 90 to 110 g protein (smaller adults or dose-escalation weeks)
- Breakfast: 1 cup nonfat Greek yogurt, half cup berries, 2 tablespoons low-sugar granola, 1 tablespoon ground flax (about 25 g protein)
- Snack: 1 stick string cheese and a small apple (about 8 g protein)
- Lunch: 4 oz grilled chicken, 1 cup mixed greens with olive oil and lemon, half cup quinoa (about 35 g protein)
- Snack: half scoop whey shake in 1 cup milk (about 20 g protein)
- Dinner: 4 oz baked salmon, half cup roasted sweet potato, 1 cup roasted zucchini and peppers (about 28 g protein)
1,500 to 1,700 kcal day, around 110 to 130 g protein (most adults at maintenance dose)
- Breakfast: 3-egg veggie omelet with spinach and feta, 1 slice sourdough toast, half cup berries (about 30 g protein)
- Snack: 1 cup low-fat cottage cheese with pineapple (about 25 g protein)
- Lunch: turkey and avocado wrap on a high-fiber tortilla, 1 cup vegetable soup (about 30 g protein)
- Snack: small handful almonds and a clementine (about 6 g protein)
- Dinner: 5 oz lean steak or grilled chicken, 1 cup roasted potatoes, 1.5 cups mixed roasted vegetables, side salad (about 40 g protein)
1,800 to 2,000 kcal day, around 130 to 150 g protein (larger adults, active patients, or maintenance after weight loss)
- Breakfast: protein oats (half cup oats, 1 scoop whey, 1 cup milk, half banana, 1 tablespoon peanut butter) (about 35 g protein)
- Snack: 1 cup skyr with berries (about 20 g protein)
- Lunch: 5 oz grilled chicken bowl with brown rice, black beans, salsa, and avocado (about 40 g protein)
- Snack: hummus with carrots and a hard-boiled egg (about 10 g protein)
- Dinner: 6 oz baked cod, 1 cup quinoa, sauteed spinach with garlic, side salad (about 45 g protein)
Vegetarian or vegan adaptation, around 100 to 120 g protein
- Breakfast: tofu scramble (6 oz firm tofu, peppers, onions, nutritional yeast), 1 slice whole-grain toast (about 25 g protein)
- Snack: soy milk latte and 1 protein bar with at least 15 g protein (about 20 g protein)
- Lunch: lentil and chickpea bowl with quinoa, roasted vegetables, tahini dressing (about 25 g protein)
- Snack: edamame with sea salt (about 17 g protein per cup shelled)
- Dinner: tempeh stir-fry with brown rice, broccoli, peppers, and peanut sauce (about 30 g protein)
Each plan can be scaled up or down by a snack, swapping a half-shake in or out, or adjusting starch portions. If you have type 2 diabetes, an insulin regimen, or chronic kidney disease, work with a registered dietitian on the specifics rather than copying these directly.
Eating out, travel, and social meals
Restaurants are where most GLP-1 patients first realize their old portions no longer fit. The simplest playbook:
- Order a protein-forward main: grilled fish, roast chicken, steak, eggs, tofu, lean cuts
- Ask for sauces, dressings, and gravies on the side and use about half what you used to
- Split entrees or take half home before you start; the slow stomach makes "I will just stop when full" less reliable than a pre-portioned plate
- Avoid stacking the bread basket plus a heavy main plus dessert; pick one
- Soup-and-half-sandwich style menus, Mediterranean mezze plates, and Japanese set meals tend to be the friendliest formats
- Skip fried appetizers and creamy dips; they hit the slow stomach hardest
- Pre-load with a small salad or broth-based soup to take the edge off appetite without filling the stomach
For business meals and conference dinners, the cleanest move is to scan the menu in advance, decide on a protein-and-vegetables plate, and commit to it before social pressure starts. A glass of sparkling water with lime or a single half-portion of wine sips slowly enough to fit in with a drinking table without putting alcohol on top of an already slow stomach.
For travel, the failure mode is not having protein available when you finally feel hungry, often after a flight or a long drive. Useful items to pack: shelf-stable protein bars (look for at least 15 g protein and under 10 g added sugar), single-serve protein powder packets, jerky, roasted chickpeas, freeze-dried Greek yogurt, instant oatmeal cups with a protein scoop. Hotels with breakfast buffets are friendly territory; aim for eggs and yogurt rather than the pastry tray. On airplanes, request water early and often, skip the carbonated drink cart, and bring a sandwich or wrap from the terminal because airline meals are usually small, salty, and not protein-dense.
Vitamins, minerals, and supplements worth considering
Sustained low intake increases the risk of running short on a handful of nutrients. People on GLP-1s for several months are sometimes light on protein, calcium, vitamin D, vitamin B12, iron, magnesium, potassium, and omega-3, particularly if dairy, meat, or produce intake has dropped sharply. [2][3][9][16] None of this is automatic; many patients eat well enough on a smaller appetite to stay sufficient. The point of the list below is to know which markers are worth checking with your provider after six months of treatment.
- Multivitamin: a standard once-daily multivitamin covers the baseline of B12, D, iron, zinc, iodine, and several others, and is the simplest single insurance policy for most patients. [16]
- Vitamin D: 1,000 to 2,000 IU daily is a common default; people who are overweight, dark-skinned, or in northern latitudes often need the higher end. Test serum 25-hydroxy D after a few months and adjust. [9][16]
- Vitamin B12: GLP-1s slow gastric emptying and can blunt B12 absorption, and the risk compounds for patients also on metformin, which independently lowers B12. [16] If you take both, B12 supplementation (a daily 500 mcg tablet or 1,000 mcg sublingual) is essentially routine.
- Calcium: aim for 1,000 to 1,200 mg per day from food plus supplements combined; protect bone density during weight loss, especially in postmenopausal women.
- Iron: only supplement if labs show low ferritin or you are menstruating with heavy periods. Iron supplements often worsen GI side effects on a GLP-1, so blood-test first rather than guessing. [16]
- Magnesium: 200 to 400 mg of magnesium glycinate or citrate at night helps with both constipation and sleep.
- Omega-3 (EPA/DHA): 1 to 2 g per day if you are not eating fatty fish twice a week.
- Whey, casein, or pea protein powder: not strictly a supplement but the single highest-yield food product for GLP-1 patients trying to land a daily protein target with a small appetite.
- Creatine monohydrate: 3 to 5 g per day. Cheap, well-studied, and one of the few supplements with consistent evidence for improved strength and lean-mass preservation when combined with resistance training. Used in published GLP-1 lean-mass case studies. [11]
- Soluble fiber supplement (psyllium): useful if you cannot land 25 to 35 g of fiber from food.
Skip anything marketed as a "GLP-1 booster" or a "natural Ozempic." None of those products outperform the basics above, and several contain stimulant laxatives that worsen the same gut side effects you are trying to avoid.
Special diets: keto, Mediterranean, intermittent fasting
GLP-1 medications are diet-agnostic, so they layer onto whatever eating pattern you already use. A few combinations are worth thinking through specifically:
- Mediterranean: probably the best-studied long-term pattern for cardiometabolic health, and it pairs naturally with GLP-1 priorities (lean protein, fish, vegetables, olive oil, legumes, whole grains, modest dairy, low ultra-processed food). Most dietitian-built GLP-1 meal plans are essentially Mediterranean with a higher protein dial. [9][12]
- Vegetarian and vegan: workable but require deliberate protein planning. Combine soy, pea, lentils, beans, and dairy or plant-protein powders to hit per-meal targets, and consider a B12 supplement (essential on a vegan diet regardless of GLP-1) and a D supplement. [13]
- Higher-protein, moderate-carb: the simplest default and what most clinical guidance points to. About 30 percent of calories from protein, 35 to 45 percent from carbohydrate (favoring fiber-rich choices), and the rest from fat.
- Ketogenic: it works for weight loss in many people, but the high fat content can worsen GLP-1-related nausea, and the very low carbohydrate intake can compound fatigue and constipation. If you want to try keto on a GLP-1, do it on a stable dose rather than during dose escalation, and lean toward leaner cuts and olive oil rather than heavy cream and butter.
- Intermittent fasting: the appetite suppression from a GLP-1 makes long fasts feel easier than they are. Most clinicians are comfortable with a 12 to 14 hour overnight fast, but more aggressive 18:6 or one-meal-a-day patterns risk under-eating protein, missing fluid, and amplifying low-blood-sugar episodes in patients who also take insulin or sulfonylureas. [17] If you want to time-restrict, set a daily protein floor first and only fast as long as you can still hit it.
- Pre-existing GERD, IBS, or gastroparesis: GLP-1s slow the stomach further, so any of these conditions deserve a conversation with the prescriber and ideally a dietitian before starting or escalating doses. Established gastroparesis is generally considered a relative contraindication. [1]
When a history of disordered eating is part of the picture
GLP-1 medications interact with eating-disorder risk in complicated ways, and it is worth being honest about that. The same biology that quiets food noise can quiet hunger cues a person with a history of restriction relied on to know when to eat. For a meaningful subset of patients, that combination can reinforce restrictive patterns and mask early relapse. [18]
Major eating-disorder organizations including ANAD and the National Eating Disorders Association recommend caution before prescribing GLP-1 medications to anyone with a history of anorexia nervosa, bulimia nervosa, atypical anorexia, or active restrictive or purging behaviors, and the Eating Recovery Center generally advises against prescribing in this population outside of specialized care. [18] Useful warning signs during treatment include rigid food rules, growing fear of specific foods, hiding meals, escalating exercise to compensate for intake, weighing more than once a day, or a sense of relief at not having to eat. If any of those creep in, loop in your prescriber and consider working with a clinician who specializes in eating disorders. Helpful starting resources include the National Eating Disorders Association helpline (1-800-931-2237 in the US), ANAD, and the Academy for Eating Disorders provider directory.
None of this means GLP-1s are off-limits for everyone with a complex food history, only that the decision and the monitoring belong with a clinician who has the full picture, not with a telehealth checkbox.
Coming off a GLP-1 (or pausing it)
When people stop a GLP-1, appetite returns, often briskly. Trial data from the STEP-1 extension showed that participants regained roughly two-thirds of the weight they had lost within a year of stopping semaglutide if no other supports were in place, and most cardiometabolic improvements reverted along with the weight. [8] That is not an argument against ever stopping; it is an argument for planning the off-ramp with the same care as the on-ramp.
Practical scaffolding that helps people land softly:
- Keep the protein-first pattern; this is the single most predictive habit for maintenance after weight loss
- Keep resistance training two to four times a week to defend the lean mass you protected during treatment
- Re-introduce higher-calorie foods deliberately, not by drift; the appetite return often arrives faster than the new normal sense of fullness
- Consider a maintenance dose with your prescriber; for some patients a lower ongoing dose is a reasonable middle path between full treatment and full discontinuation
- Weigh weekly rather than daily, and treat any 5-pound regain as a signal to tighten the basics rather than as a failure
- Stay in some form of follow-up; people who stay connected to a clinician, dietitian, group, or coach maintain weight loss substantially better than people who go it alone
The eating skills built during treatment are what carry the result forward. The medication is a tool that made those skills easier to install; off the medication, the skills still work, but the appetite headwind is back, and that is the variable to plan for.
References
- National Institute of Diabetes and Digestive and Kidney Diseases. Prescription Medications to Treat Overweight & Obesity. NIDDK, 2023. niddk.nih.gov
- Wilding JPH, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine. 2021;384:989-1002. doi:10.1056/NEJMoa2032183
- Conte C, et al. Multiorgan effects of glucagon-like peptide-1 receptor agonists in obesity: implications for body composition and lean mass. Nutrients. 2024;16(11):1668. PMID: 38892559
- Phillips SM, Chevalier S, Leidy HJ. Protein "requirements" beyond the RDA: implications for optimizing health. Applied Physiology, Nutrition, and Metabolism. 2016;41(5):565-572. PMID: 26960445
- Harvard Health Publishing. GLP-1 diabetes and weight-loss drug side effects: "Ozempic face" and more. Harvard Medical School, 2024. health.harvard.edu
- Cleveland Clinic. GLP-1 Agonists. Cleveland Clinic, 2024. clevelandclinic.org
- Quddos F, et al. Semaglutide and Tirzepatide reduce alcohol consumption in individuals with obesity. Scientific Reports. 2023;13:20998. PMID: 38017205
- Wilding JPH, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes, Obesity and Metabolism. 2022;24(8):1553-1564. PMID: 35441470
- Academy of Nutrition and Dietetics. Position Paper: Interventions for the Treatment of Overweight and Obesity in Adults. Journal of the Academy of Nutrition and Dietetics. 2016;116(1):129-147. PMID: 26718656
- Locatelli JC, et al. Incretin-Based Weight Loss Pharmacotherapy: Considerations for Skeletal Muscle Mass and Functional Capacity. Diabetes Care. 2024;47(10):1718-1730. PMID: 38687506
- Preservation of lean soft tissue during weight loss induced by GLP-1 and GLP-1/GIP receptor agonists: a case series. PMC, 2024. PMC12536186
- Cleveland Clinic Health Essentials. Can Certain Foods Impact Your Ozempic Side Effects? (Beth Czerwony, RD, LD). 2024. health.clevelandclinic.org
- Academy of Nutrition and Dietetics. Plant-Based Diet Position Paper. Journal of the Academy of Nutrition and Dietetics. 2016;116(12):1970-1980. PMID: 27886704
- Healthline. Ozempic Diet Plan: A List of Foods to Eat and What to Avoid. 2024. healthline.com
- Hendershot CS, et al. Once-Weekly Semaglutide in Adults With Alcohol Use Disorder: A Randomized Clinical Trial. JAMA Psychiatry. 2025. PMID: 39937469
- Medical News Today. What vitamins to take with Ozempic (semaglutide) and why. 2024. medicalnewstoday.com
- Klinic. Combining Intermittent Fasting with GLP-1 Medications: Safety Considerations. 2024. klinic.com
- National Association of Anorexia Nervosa and Associated Disorders (ANAD). GLP-1 Medications & Eating Disorders. anad.org