Exercise & Lifestyle on GLP-1
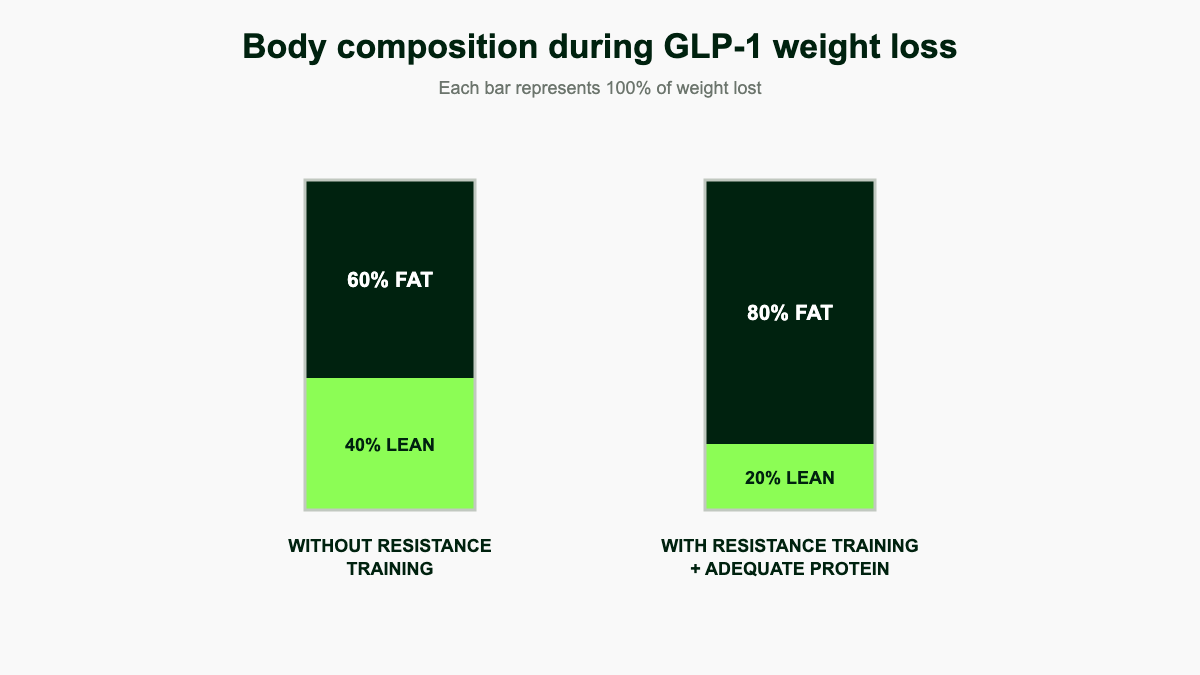
Summary: Roughly a quarter of the weight you lose on a GLP-1 is lean tissue if you do nothing about it. Resistance training two to three times per week, adequate protein, daily walking, and decent sleep are the levers that turn drug-driven weight loss into a leaner, stronger body.
This content is for informational purposes only and is not medical advice. Always consult a qualified healthcare provider before starting, changing, or stopping any medication.
The lean mass problem with rapid weight loss
Any large, fast drop in body weight strips off muscle along with fat. That is true of bariatric surgery, very-low-calorie diets, and GLP-1 medications like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound). The drug is not directly catabolic to muscle. The problem is the energy deficit it creates: appetite drops, intake falls, and without a strong stimulus to keep skeletal muscle, the body lets some of it go. [1][2]
This matters for several reasons. Muscle drives resting metabolic rate, so losing it makes long-term weight maintenance harder. A roughly 10% drop in lean mass over 18 months is comparable to what most adults lose across a decade or more of normal aging, which means a 50-year-old finishing a year on tirzepatide may walk out of the deficit with the appendicular muscle of someone in their early 60s if no countermeasure is in place. [13] Strength and lean mass predict physical function and independence as you age, and the lean tissue you lose during weight loss is not guaranteed to come back when you stop the medication, especially if training does not change.
For older adults the stakes climb further. Sarcopenic obesity, the combination of high body fat and low muscle mass or function, already affects roughly 20% of treatment-seeking adults with obesity. Repeated cycles of GLP-1 therapy and discontinuation can pull body composition closer to that profile, since regained weight is mostly fat while lost muscle is harder to put back. [14] The bright side: nothing about a GLP-1 forces this outcome. The drug is appetite-neutral toward training adaptation. What you eat, how you move, and how you sleep during the deficit decide the body composition that comes out the other side.
Why GLP-1 weight loss is different from a regular diet
Self-directed dieting tends to be slow and incomplete. People stall around 5 to 8% body weight and either give up or plateau. GLP-1 therapy creates a deeper, more sustained deficit because hunger and food noise drop simultaneously. That is great for fat loss numbers and disease risk, but the same mechanism removes most of the body's protective signals against under-eating: you simply do not feel hungry on a 1,200-calorie day, even if you need 1,800. Without conscious targets for protein, training, and total intake, the body is left to defend itself against an energy drop it cannot complain about.
This is why frameworks built for old-school dieting (move more, eat less) underperform here. The right framing is closer to a managed surgical recovery: appetite and food intake are no longer your warning system, so other metrics (protein grams, training sessions, daily steps, sleep hours, strength PRs, energy levels) become the dashboard you check.
What the trials actually show
The numbers are consistent across major trials and useful for setting expectations.
- STEP 1 body composition substudy (semaglutide 2.4 mg, n=140). Total body weight fell 15.0% versus 3.6% on placebo. Fat mass dropped 19.3% and visceral adipose tissue dropped 27.4%. Lean body mass dropped 9.7%. The lean-to-fat ratio improved from 1.34 to 1.57, meaning body composition still got better even though lean mass came down in absolute terms. Among participants who lost 15% or more of body weight, the lean-to-fat ratio improved by 0.41; below that threshold the ratio improvement was only 0.03, which suggests that bigger losses produce a more favorable composition shift overall. [3]
- SURMOUNT 1 body composition substudy (tirzepatide, n=160). Fat mass fell 33.9% (-15.9 kg) and lean mass fell 10.9% (-5.6 kg) over 72 weeks. Visceral fat mass fell 40.1% and waist circumference dropped 18.1 cm. Approximately 75% of the weight lost was fat and 25% was lean tissue, a ratio that held steady across age, sex, and weight loss tertiles, with a slight trend toward more favorable composition (76% fat) in the highest weight-loss tertile. [4]
- Systematic review of semaglutide trials (1,541 adults across 6 studies). Lean mass reductions ranged from near zero up to about 40% of total weight lost, with larger reductions seen in larger trials. The proportion of lean mass relative to total body mass typically increased, but absolute losses were real. [5]
- Locatelli narrative review (Diabetes Care 2024). Across the incretin family, the typical lean mass loss is roughly 6 kg, comparable to a decade or more of normal aging. The same review noted that 10+ weeks of supervised resistance training in adults can add about 3 kg of lean mass and a 25% strength increase, which is more than enough to neutralize the medication-side losses. [13]
The takeaway: expect roughly 25 to 40% of your weight loss to come from lean tissue if you change nothing. Structured resistance training and adequate protein consistently shrink that fraction, often to under 15% of total weight lost. The trial averages reflect what happens to mostly sedentary participants who were not given a structured exercise prescription. They are not a ceiling.
Resistance training is the main lever
Aerobic exercise is excellent for cardiovascular and metabolic health, but resistance training is what tells the body to keep skeletal muscle during an energy deficit. The mechanism is mechanical tension. When a muscle works against load close to its capacity, it produces a signal (largely through mTOR-pathway activation) to maintain or build contractile protein. That signal partially offsets the proteolytic drift that an energy deficit would otherwise produce. Combine it with adequate dietary protein and the body has both the order and the raw materials to keep muscle around. [6][13]
Practical targets supported by ACSM, Locatelli et al., and the broader hypertrophy literature:
- Frequency: 2 to 4 full-body sessions per week, 30 to 60 minutes each. More is fine if you recover well; less than two is the floor. The Locatelli review specifically recommends two to three weekly sessions with at least seven exercises targeting large muscle groups. [13]
- Volume: roughly 10 to 20 hard sets per muscle group per week, distributed across sessions. The dose-response curve for hypertrophy rises steeply through 10 sets per muscle per week and starts to flatten beyond 20.
- Intensity: 50 to 85% of your one-rep max, or roughly RPE 7 to 9 (you could do 1 to 3 more clean reps if forced). Newer or older lifters anchor toward 50 to 70%; experienced lifters can push the upper end safely.
- Reps: 5 to 15 reps per set works well for hypertrophy and strength. The last one to three reps should feel genuinely hard.
- Progression: add weight, reps, or sets over time. Doing the same 3-pound dumbbells for six months will not preserve muscle. A small notch up every one to three weeks is enough.
- Movement selection: compound lifts give the most return per minute. Squat, hinge, push, pull, carry. Add isolation work (curls, lateral raises, leg curls) only after the compound base is in place.
- Rest between sets: 90 to 180 seconds for compound lifts, 60 to 90 seconds for isolation work. Cutting rest short to "make it harder" usually trades load for fatigue and slows progress.
The single most common mistake on a GLP-1 is trying to compensate for low energy by lifting smaller weights for higher reps. The body responds to load. If your training never feels heavy, it never gets the signal it needs to keep muscle.
Sample weekly templates
You do not need a complicated split. The four templates below cover the realistic range from "never trained before" to "already lifting four days a week before the prescription."
Template 1: Brand-new lifter, full body 2 days per week
Best for someone who has never been to a gym, is on a starting dose, or is dealing with significant GI side effects. The goal is consistency and movement quality, not heroics.
- Day A (Mon or Tue): Goblet squat 2x8, incline push-up 2x8-12, supported one-arm row 2x10, sit-to-stand 2x10, walk 15 to 20 min.
- Day B (Thu or Fri): Romanian deadlift with light dumbbells 2x8, seated overhead press 2x8, lat pulldown or band row 2x10, glute bridge 2x12, walk 15 to 20 min.
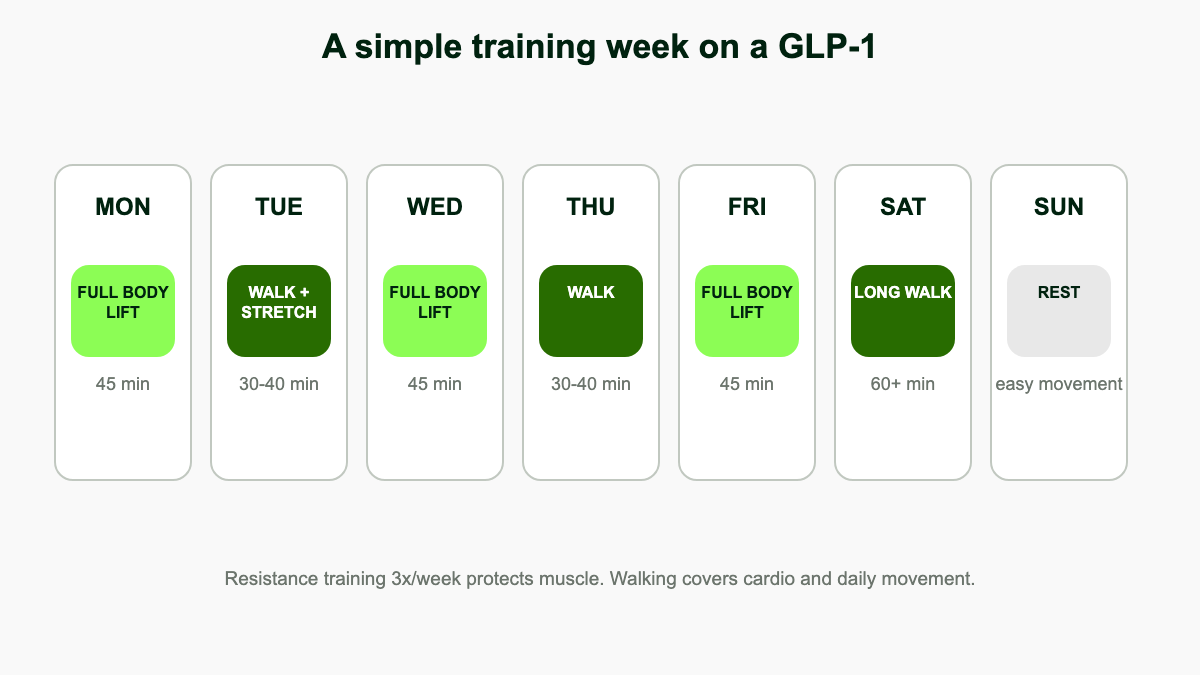
Template 2: Beginner, full body 3 days per week
The default recommendation for most adults on a GLP-1 who can train safely.
- Day A (Mon): Goblet squat 3x8, dumbbell bench or push-up 3x8-12, one-arm row 3x10, plank 3x30s, walk 20 min.
- Day B (Wed): Romanian deadlift 3x8, overhead press 3x8, lat pulldown or assisted pull-up 3x8-10, dead bug 3x10, walk 20 min.
- Day C (Fri): Leg press or split squat 3x10, incline dumbbell press 3x10, seated row 3x10, farmer carry 3x40 steps, walk 20 min.
Template 3: Intermediate, upper/lower 4 days per week
For people who already train and want a clearer division between leg and upper-body recovery.
- Lower A (Mon): Back squat 4x5, Romanian deadlift 3x8, walking lunge 3x10/leg, leg curl 3x10, calf raise 3x12.
- Upper A (Tue): Bench press 4x6, one-arm dumbbell row 4x8, overhead press 3x8, lat pulldown 3x10, biceps curl 2x12.
- Lower B (Thu): Front squat or hack squat 3x8, hip thrust 3x10, Bulgarian split squat 3x8/leg, hamstring curl 3x12, plank 3x45s.
- Upper B (Fri): Incline dumbbell press 4x8, chest-supported row 4x10, dumbbell shoulder press 3x10, face pull 3x12, triceps pushdown 2x12.
Template 4: Push/pull/legs, 6 days per week
For experienced lifters who already had a six-day routine in place. Most people on a GLP-1 do better at three or four days, but if recovery and fueling are dialed in, this volume is sustainable.
- Push 1, Pull 1, Legs 1, rest, Push 2, Pull 2, Legs 2. Two pressing movements, two pulling movements, and two leg movements per session, 3 to 4 sets each, mixing 5 to 8 rep "strength" work with 8 to 12 rep "growth" work.
Bodyweight-only adaptation
If you do not have access to weights, the same logic applies but you progress by moving from easier to harder variations rather than adding plates. Push-ups: incline, then standard, then deficit, then archer. Squats: chair-supported, then air squat, then split squat, then pistol progressions. Rows: door-frame inverted rows or band rows. Hinges: single-leg deadlift, glute bridge, then hip thrust. Aim for two hard sets per movement, two to three days per week, and find ways to keep adding difficulty.
Home gym minimal equipment
A pair of adjustable dumbbells (5 to 50 lb), a bench, and a pull-up bar covers 90% of what you need. Add resistance bands for assistance pull-ups, lateral raises, face pulls, and travel.
Whichever template you pick, rest 60 to 180 seconds between sets, log your weights, and add a small amount of load or one extra rep when a set feels easier than usual. If you can hire a coach for four to six weeks, use it. Form on squats, hinges, and pressing movements pays back for years.
Cardio: useful, but secondary
Cardio is not the primary tool for body composition during GLP-1 use, but it earns its place for heart health, blood pressure, sleep, and appetite regulation. The Physical Activity Guidelines for Americans recommend roughly 150 minutes per week of moderate-intensity aerobic activity, or 75 minutes of vigorous activity, plus two days of resistance training. [7] On a GLP-1, that floor is easy to hit and comfortable to exceed.
The trap is doing so much cardio that it crowds out resistance training or eats into already-low intake. Long Saturday runs feel productive and burn calories, but they do nothing for the lean-mass problem and can leave you too tired to lift well on Monday. A useful split for most people: 2 to 3 resistance sessions per week, 1 to 2 moderate cardio sessions of 20 to 40 minutes, and daily walking on top.
Choose between formats by joint and recovery cost. Low-intensity steady state (LISS) such as brisk walking, easy cycling, swimming, or rowing is forgiving on joints and easy to recover from, which makes it the right default for older adults, anyone with knee pain, or weeks where training is hard. High-intensity interval training (HIIT) is metabolically efficient but expensive on recovery, especially during dose escalations. Keep HIIT modest in the first weeks of a new dose. GI side effects can flare with hard efforts, particularly on injection day. [8]
For people with cardiovascular indications, the picture sharpens. Cardiac rehabilitation programs that combine GLP-1 therapy with structured aerobic training have shown reduced major adverse cardiovascular events and improved exercise capacity, especially in HFpEF and post-MI populations. If your cardiologist has cleared aerobic exercise, the GLP-1 makes the program easier to adhere to, not harder. [15]
Walking and daily movement: the underrated lever
Walking deserves its own section because it is the cheapest, lowest-risk, highest-leverage thing most GLP-1 users can do. It has near-zero recovery cost, tends to settle GI side effects rather than worsen them, and adds meaningful daily energy expenditure without driving appetite up.
A reasonable target is 7,000 to 10,000 steps per day, or simply 2,000 more than your current baseline. Mortality risk drops sharply between roughly 4,000 and 8,000 steps per day in adults over 60, and continues to fall up to about 10,000 in younger adults, with diminishing returns after that. A 10 to 20 minute walk after your largest meal also blunts post-meal glucose spikes by 15 to 30 mg/dL in adults with prediabetes, and short post-meal walks tend to outperform a single longer walk for 24-hour glucose control.
The other reason walking matters is non-exercise activity thermogenesis (NEAT): the calories you burn fidgeting, taking stairs, doing chores, and generally not sitting. NEAT can vary by 2,000 calories per day between two people of the same weight, and during weight loss it tends to drop as the body unconsciously reduces small movements to defend bodyweight. [16] That adaptive drop is one of the main reasons people regain weight even when they "ate the same." Deliberately keeping movement in your day (standing desk, walking meetings, parking farther, taking the stairs, a 10-minute loop after dinner) replaces what your body would otherwise quietly cut.
Concrete habits that work: a fixed morning walk of 15 to 30 minutes, a 10-minute post-lunch loop, a 10-minute after-dinner walk, and either commuting on foot for one segment of the day or installing a standing desk. Together those add 5,000 to 8,000 steps without requiring a workout.
Protein targets for trained individuals on GLP-1
Protein is the single most important nutritional variable for preserving muscle in a deficit. The relevant comparison isn't the RDA (0.8 g/kg) but the higher targets used in athletic and weight-loss research, where 1.2 to 1.6 g/kg/day reliably outperforms lower intakes for lean mass preservation. Studies that pushed intake to 2.4 g/kg saw no extra benefit beyond 1.6, so 1.6 is a sensible operating target with 1.2 as the floor. [9][17]
Practical translations:
- Default target: 1.2 to 1.6 g/kg body weight (roughly 0.55 to 0.73 g/lb) per day. For a 90 kg / 200 lb adult, that is 110 to 145 g daily. If you have a lot of fat to lose, anchor to ideal or "goal" body weight rather than current weight so the target stays achievable.
- Distribution: 30 to 50 g of high-quality protein at each of 3 to 4 meals stimulates muscle protein synthesis more reliably than two large doses. Older adults benefit from the higher end (40 to 50 g per meal) due to anabolic resistance.
- Sources that work on a low appetite: Greek yogurt, eggs, cottage cheese, chicken, fish, tofu, edamame, lean ground turkey or beef, shrimp. Liquid options (whey isolate, casein, plant blends) often go down easier than solids on rough days.
- Eat protein first. Start meals with the protein source while appetite is still present. The fiber and fat that fill you up later will not displace something already eaten.
- Creatine: 3 to 5 g of creatine monohydrate per day is a low-cost addition with strong evidence for muscle, strength, and even cognition. It causes a small water-weight increase (1 to 2 lb) that some people misread as fat gain. Skip if you have known kidney disease. [18]
Fueling around training
Workout-day nutrition matters more on a GLP-1 than off it, because there is less margin to absorb a missed meal. Aim to have something in your system before you train, even if appetite is flat.
- Pre-workout (60 to 90 min before): 20 to 30 g protein with 20 to 40 g of easy carbohydrate. A scoop of whey in milk plus a banana, Greek yogurt with honey and berries, or oats with protein powder. Liquids work when solids don't.
- Intra-workout: water with electrolytes for sessions over 45 minutes or in heat. Sip throughout rather than chugging at the end.
- Post-workout (within 2 hours): 25 to 40 g of high-quality protein with mixed carbs and a little fat. A real meal is fine; a shake plus fruit is fine; both is better.
- Hydration: 2 to 3 liters of fluids daily, more in heat or with longer sessions. Add sodium, potassium, and magnesium if you sweat heavily or have had nausea, vomiting, or loose stools. Dehydration amplifies dizziness and GI symptoms. [1][8]
Energy management when appetite is low
Some weeks the medication will leave you genuinely uninterested in food. The mistake is to treat that as permission to eat almost nothing and assume the body will handle it. The body handles it by pulling apart muscle. The fix is to switch from "eat by appetite" to "eat by the clock," at least on training days.
- Build a non-negotiable minimum: three to four protein-anchored eating moments per day at fixed times, regardless of hunger. A 30 to 40 g protein shake is an eating moment.
- Use liquid calories on rough days: smoothies with protein powder, frozen fruit, oats, and a spoon of nut butter often go down when food won't. A 600 to 800 calorie shake takes 90 seconds to drink.
- Adjust training, not protein: if peak GI symptoms are wrecking sessions in the first week of a new dose, drop training volume by a third (fewer sets, lighter loads) but keep showing up. Protein and steps stay constant.
- Keep emergency protein in the house: ready-to-drink shakes, jerky, hard-boiled eggs, cottage cheese cups. Decision fatigue is the enemy on low-appetite days.
Sleep and recovery
Sleep restriction blunts the muscle-preserving response to training and shifts weight loss toward lean tissue rather than fat. Adults losing weight while sleeping less than about 5.5 hours per night lose a substantially smaller share of their weight as fat compared with those getting 8.5 hours. The practical floor is 7 hours; aim for 7 to 9 with consistent timing. [10]
The good news for sleep on a GLP-1: weight loss itself improves sleep quality, and tirzepatide in particular has direct evidence for sleep apnea improvement. In SURMOUNT-OSA, tirzepatide reduced the apnea-hypopnea index by up to 58.7% from baseline (versus 3% on placebo) and brought 43 to 51.5% of participants below the threshold for clinically significant OSA. [19] If your sleep has been poor because of OSA, expect that to improve as weight comes off, and consider a follow-up sleep study after meaningful weight loss to recheck CPAP needs.
Recovery suffers when total intake is low. Signs you are under-fueling: persistent soreness past 72 hours, declining session performance, low mood, hair shedding, cold hands and feet, irregular menstrual cycles, and rising resting heart rate. The fix is usually more protein and more total calories on training days, not more training. Stress management matters too; chronically elevated cortisol from poor sleep, work pressure, or under-eating amplifies muscle loss and undermines fat loss.
The mental side and adherence
The mental side is real and underdiscussed. Many people on GLP-1s report a quieter "food noise" that makes the gym easier to attend, since a workout no longer competes with constant cravings. Use that window. Build the habit while the medication makes adherence easier, so the routine survives once you taper or stop.
Body image during a rapid composition change can be unexpectedly difficult. Clothes fit differently, mirrors look unfamiliar, and family members often comment in ways that miss the mark. Anchor identity in things you can do (grip strength, weight on the bar, distance walked, sleep quality, energy at 4 p.m.) rather than only the number on the scale. Strength PRs and a heavier deadlift are concrete, repeatable wins that stick around even when the scale plateaus.
Going to the gym while undereating creates its own mental drag. If a session feels hopeless, do the warm-up and one working set of two compound lifts, then leave. Showing up is the adaptation that matters most.
Specific scenarios
The general framework holds across people, but a few situations deserve their own notes.
- Brand new to exercise. The first six weeks are about consistency, not load. Use machines or supported variations, learn the squat / hinge / push / pull pattern, and do two short sessions per week before adding a third. Injury risk is highest when an enthusiastic but deconditioned body meets a gym.
- Returning after a long sedentary stretch. Start at roughly 50 to 60% of what you used to lift. Tendons recover slower than muscle, and the temptation to chase old numbers in week two reliably produces tendinitis by week six.
- Already an athlete. Most lifters and runners can keep their training intact through GLP-1 use, with two adjustments: front-load nutrition around hard sessions, and accept that PRs may be slower to come during the deepest deficit. Maintenance is the win in this phase.
- Older adults (65+). Resistance training plus protein matters most for this group because the cost of further muscle loss is functional decline. Add balance work (single-leg stands, heel-to-toe walks, tai chi) and consider creatine 3 to 5 g/day. [18][14]
- Knee or hip osteoarthritis. Many GLP-1 users already have OA from years of carrying extra weight. Weight loss itself reduces joint load, and the TRIUMPH-4 trial of retatrutide showed up to a 75.8% reduction in WOMAC knee pain at the highest dose. [20] Pick movements that stay pain-free: leg press, hack squat, sled push, hip thrust, and step-ups often work when free squats do not. Cycling and swimming as cardio.
- Cardiac rehab populations. Train within the heart-rate or RPE limits set by your program. The combination of GLP-1 plus structured cardiac rehab is well tolerated and improves outcomes. [15]
- Pregnancy and trying to conceive. GLP-1 medications are not recommended during pregnancy or while trying to conceive; many guidelines suggest stopping at least two months before. Continue moderate exercise per OB guidance, but the drug-driven framing of this article does not apply. Discuss with your clinician.
Tracking the right metrics
The scale alone is a bad dashboard during GLP-1 weight loss because it cannot tell you whether you lost fat or muscle. Layer in a few more signals.
- DXA scan every 6 to 12 months. The most accurate way to see fat mass, lean mass, and visceral fat trends. Cost is typically $50 to $150 in the US. One baseline scan and one follow-up at 6 months tells you whether the protein and training plan is working.
- Bioimpedance scales. Less accurate but cheap and trendable. Track the direction over weeks rather than any single reading; hydration changes the number more than fat does.
- Tape measurements. Waist, hips, thigh, and upper arm every 4 weeks under the same conditions. Waist below half your height is a useful long-term target.
- Strength PRs. Log every working set. If your top set on three core lifts (squat or leg press, press, row or pull) is going up or holding while body weight drops, lean mass is in good shape.
- Function tests. 30-second sit-to-stand count, grip strength with a $25 dynamometer, and a one-mile walk time. Improvements here predict long-term health better than scale changes.
- Photos. Same lighting, same angles, same clothes, every 4 weeks. Faster to interpret than any number.
Red flags and when to slow down
Not every bad week is a problem, but a stack of these signals together is a reason to back off training, raise intake, and check in with your clinician.
- Persistent fatigue that does not lift after a rest day or a bigger eating day.
- Strength dropping for two or more consecutive weeks across multiple lifts.
- Resting heart rate trending up by 5+ beats per minute over a couple of weeks.
- Loss of menstrual cycle or significant cycle irregularity in premenopausal women.
- Worsening sleep, vivid dreams, early waking, or frequent night-time waking.
- Hair shedding, brittle nails, persistently cold hands and feet.
- Lightheadedness on standing, palpitations, or fainting (also check hydration and electrolytes urgently).
- Mood changes: low motivation, persistent low mood, or unusual irritability.
The first response to almost all of these is more food (especially protein and carbs) and less training, in that order. The second response, if symptoms persist, is a clinician visit to check labs and discuss whether the dose, the rate of weight loss, or the plan needs to change.
What to do if you stop the medication
Weight regain after stopping a GLP-1 is well documented. In a withdrawal substudy of semaglutide, participants who came off the drug regained roughly two-thirds of the weight lost within a year. [11] What you do with training and protein during the off-ramp matters more than the off-ramp itself.
- Keep training at the same frequency. Two to three resistance sessions per week is the maintenance dose.
- Hold protein intake steady or slightly higher. Appetite will return; protein-first habits prevent that hunger from being absorbed entirely by refined carbs.
- Watch the scale weekly, not daily. A 2 to 3 kg upward drift is normal; a 5+ kg drift over a few months is a signal to revisit your plan with your clinician.
- Keep walking. Daily steps are the easiest expenditure to keep when life gets busy.
Putting it together
Treat the medication as the part of the plan that handles appetite and intake. Treat training, protein, walking, and sleep as the part that decides what kind of body you end up with. The trial-average outcome (roughly 25 to 40% of weight lost coming from lean tissue) describes what happens when nothing else changes. With two to four resistance sessions per week, 1.2 to 1.6 g/kg of protein distributed across meals, 7,000 to 10,000 daily steps, and 7 to 9 hours of sleep, that fraction reliably drops into the 10 to 15% range, which is closer to "normal weight loss" than to "drug-driven sarcopenia."
None of this requires elite execution. It requires a small set of habits done consistently while the medication is doing the heavy lifting on appetite. Build them now while the drug makes adherence easier, and they will carry you through whatever comes after.
References
- Cleveland Clinic. Ozempic and Muscle Loss: What To Know. health.clevelandclinic.org/ozempic-muscle-loss
- Bikou A, et al. A systematic review of the effect of semaglutide on lean mass: insights from clinical trials. Expert Opin Pharmacother. 2024;25(5):611-619. PMID: 38629387.
- Wilding JPH, et al. STEP 1 body composition substudy: Effects of semaglutide 2.4 mg on body composition in adults with overweight or obesity. Diabetes Obes Metab. PMC8089287.
- Look AHEAD/SURMOUNT-1 body composition substudy. Body composition changes during weight reduction with tirzepatide in adults with obesity. Diabetes Obes Metab. 2025. PMID: 39996356.
- Bikou A, et al. (systematic review, 1,541 adults across 6 trials). Expert Opin Pharmacother. 2024.
- American College of Sports Medicine. Position stand on resistance training and progression models in adults; protein recommendations for active adults (1.2-2.0 g/kg/day). acsm.org
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed. 150 min/week moderate aerobic + 2 days/week resistance training. health.gov/paguidelines
- SingleCare. Working out on Ozempic: side effects, hydration, and intensity considerations. singlecare.com/blog/ozempic-and-exercise
- Phillips SM, Van Loon LJC. Dietary protein for athletes and during weight loss: from requirements to optimum adaptation. J Sports Sci. 2011;29(S1):S29-S38.
- Nedeltcheva AV, et al. Insufficient sleep undermines dietary efforts to reduce adiposity. Ann Intern Med. 2010;153(7):435-441.
- Rubino D, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance (STEP 4). JAMA. 2021;325(14):1414-1425.
- Heymsfield SB, et al. Effect of Tirzepatide on Skeletal Muscle Mass in Adults With Obesity. PMC12394919.
- Locatelli JC, et al. Incretin-Based Weight Loss Pharmacotherapy: Can Resistance Exercise Optimize Changes in Body Composition? Diabetes Care. 2024;47(10):1718-1730. PMID: 38687506.
- Prado CM, et al. Weighing the risk of GLP-1 treatment in older adults: should we be concerned about sarcopenic obesity? Eur Geriatr Med / Diabetes Metab. 2025. PMID: 40819408.
- Cardiac rehabilitation and GLP-1 receptor agonists: outcomes in real-world cohorts and HFpEF subpopulations. JACC / Circulation. 2025-2026.
- Levine JA. Non-Exercise Activity Thermogenesis (NEAT). Endotext / Mayo Clinic Proceedings. NCBI NBK279077.
- Morton RW, et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br J Sports Med. 2018;52(6):376-384.
- Candow DG, et al. Creatine monohydrate supplementation for older adults and clinical populations. J Int Soc Sports Nutr. 2025. PMC12272710.
- Malhotra A, et al. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity (SURMOUNT-OSA). N Engl J Med. 2024;391:1193-1205. PMID: 38912654.
- Eli Lilly. TRIUMPH-4: Retatrutide reduces weight and knee osteoarthritis pain in adults with obesity and OA, Phase 3 results. 2025. Investor release and HCPLive coverage.